Shredded intestines from a gunshot wound to the leg!
This is a case study of a casualty that I was involved with a number of years ago in Afghanistan. I feel it is worth sharing due to the fact that it was initially a bit of a perplexing case, however applying common Advanced Life Support principles allowed us to identify the life-threatening injury and deal with it appropriately.
The back story to the case is a bit of a mystery. The details of the gunfight in which the casualty sustained his wounds were never revealed to us, but the information we did receive was that he was brought to a remote US base in Afghanistan suffering multiple gunshot wounds to his legs. On first medical review he was haemodynamically stable, and it was initially thought that his wounds were relatively minor through-and-through gunshot wounds to the thighs. Whilst being medically reviewed at the remote base the casualty began to show increasing signs of shock, prompting an aeromedical evacuation to the Forward Surgical Team (FST) that I happened to be working with on that day. The medic at the remote base had inserted an intraosseous cannula into the casualty’s left tibia and infused 1 litre of saline before the AME arrived.


(If anyone’s interested in a more detailed look at intraosseous devices please see my previous blog post Drilling shins to save skins: demystifying intraosseous cannulation linked here.)
The casualty received two units of O-type Packed Red Cells in flight, and despite the fluids and blood was deeply shocked on arrival at the FST. On first review he appeared to have two separate through-and-through gunshot wounds to his left thigh, and what appeared to be an exit wound on his right lateral thigh. He had clearly been shot multiple times, but had no obvious wounds above his upper-thigh. He didn’t have any signs of arterial bleeding from any of his wounds, and his pulses were present, but faint, in both of his feet, implying that his femoral arteries were intact.


It appeared on initial assessment that one of the bullets had passed through the casualty’s left leg first, and then through his right leg, to account for the apparent exit wound on his right lateral thigh. A closer examination of the casualty’s inner right thigh revealed no entrance wound to support this theory, leading us to explore the possibility that the right thigh wound was in fact an entrance wound and that the bullet was still within the casualty.
With no external massive haemorrhage to deal with, we moved on with the primary survey of the casualty. His airway was patent and his breathing was rapid, but equal on both sides. He didn’t have any chest signs to suggest a tension pneumothorax or a massive haemothorax to account for his shock. Moving on with the assessment, the casualty’s abdomen was found to be slightly distended and, whilst he had a reduced conscious state due to his shock, he appeared to be in pain when his abdomen was palpated. A FAST scan was performed and revealed significant amounts of free fluid in the abdomen and pelvis.
This was a good illustration of the Blood on the floor plus four places more rhyme to help prompt us to go looking in the likely areas for massive bleeding in a shocked casualty when there is no overt sign of blood loss (i.e.: no blood on the floor). The remaining areas where a significant amount of blood can be lost are as follows:
- The thoracic cavity
- The abdomen
- The pelvis
- Around the long bones – especially the femurs
As can be seen in the photos above, although the casualty had gunshot wounds to both thighs, he doesn’t have the sort of swelling and bruising to suggest significant blood loss from fractured femurs. The bleeding responsible for his shock was in his abdomen or pelvis, and the next step was to take him to theatre and open him up to identify and treat the bleeders.
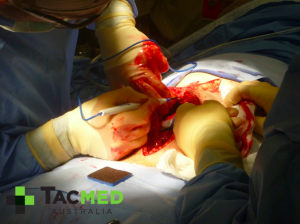
Immediately upon opening the casualty’s abdomen at laparotomy we found a significant amount of blood in his abdominal cavity, and inspection of his small intestine revealed approximately a dozen neat holes punched through it by a bullet. The offending bullet was found lodged in the underside of the casualty’s diaphragm on the left hand side, completely intact.




The approximate path of the bullet is illustrated on the following picture (picture used for adaption courtesy of fotosearch.com). The shape and size of the entrance wound on the right outer thigh would imply that the bullet may have been yawing, or tumbling, by the time it hit the casualty. This pattern may represent that the bullet was coming towards the end of its trajectory by the time of impact and had become unstable in flight. The fact that the bullet remained completely intact and minimally deformed also supports the theory that it was travelling at a relatively low velocity at impact. (For a detailed discussion of the wounding patterns of different velocity projectiles see my previous blog article Why I’d rather be shot by an AK47 than an M4 . That said, the bullet still had enough kinetic energy to plough through about a metre of soft tissues before coming to rest, and had inflicted wounds that would have killed the casualty if he hadn’t got to surgery in a timely fashion. X-rays and surgical exploration showed that the bullet had not struck any bone on its path through the body, and it had also missed the vital organs including the liver, spleen, and stomach.

After a few hours of cutting and pasting we were able to stop all the small bleeders and remove all the damaged sections of bowel, reconnecting the small intestine as not to require a stoma.


An incidental finding was a gut full of intestinal worms. This was a universal finding at laparotomy in local nationals in Afghanistan, and whilst it was the least of the casualty’s concerns at the time, the chronic effects of malnutrition and anaemia caused by the worm infestation would mean a more significant impact from blood loss and slower recovery times.

The casualty recovered well in the immediate post-operative period, then was transferred to another facility a few days later and I lost track of his long-term recovery.
This case illustrates the fact that once a missile of any description, especially a high-velocity missile, enters the body, it can end up literally anywhere and do all manner of damage without obvious external signs. The case also illustrates that if a casualty is shocked following trauma and there’s no blood on the floor then you need to go looking in the four places more. In that setting, sound clinical examination will reveal blood loss around the long bones, and should give a good indication of significant bleeding into the chest (decreased air entry and dullness to percussion on the effected side). Chest x-ray, if available, will also aid in this diagnosis. If there’s no obvious significant blood loss into the tissues around the long bones and the chest examination is unremarkable then the blood is being lost into the pelvis or the abdomen. A FAST scan will reveal this, and if so, the casualty needs a surgeon quickly. In the pre-hospital setting where a FAST scan is not available, intra-abdominal and intra-pelvic bleeding should be assumed until proven otherwise, and minimising time to surgery is crucial. A pelvic splint should be applied if a fractured pelvis is suspected, and strong arguments can be made for TXA use and permissive hypotension (but they’re topics of a whole different discussion!).
Finally, there are other rarer causes of shock following trauma, but they make up the fine print and blood loss should be assumed until proven otherwise.
As always, comments and questions are welcome. Kind regards, dan.


